The MCL is a structure that stabilizes the medial side (inside) of the knee, connecting the thigh bone (femur) to the shinbone (tibia). The MCL prevents forces applied to the lateral (outside) side of the knee from gapping open the inside of the knee (valgus stress).
The posteromedial corner of the knee is comprised of the MCL and the posterior oblique ligament (POL). Both structures control the stability and valgus stress of the knee.
The MCL and the POL prevent the knee from gapping open when the tibia internally rotates. The MCL functions when the knee is slightly flexed (20 to 30 degrees of flexion) whereas the POL (more to the back of the knee) functions close to extension (0 degrees of flexion). The different roles of each of these ligaments help to ensure the stability of the knee to valgus stress throughout a full range of motion.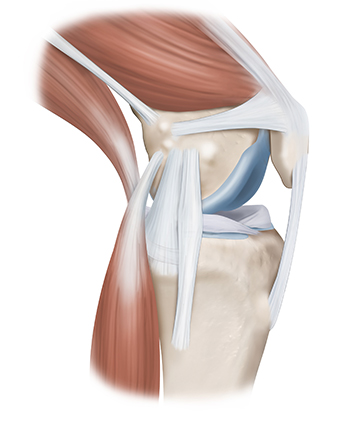
MCL injuries can result from twisting injuries, causing the knee to buckle and gap open on the inside of the knee. MCL injuries can also result from contact injuries, like a blow to the outside of the knee, causing valgus gapping. MCL injuries are very common with almost 750,000 injuries occurring every year in the United States. Overall, MCL tears are two to three times more common than ACL tears.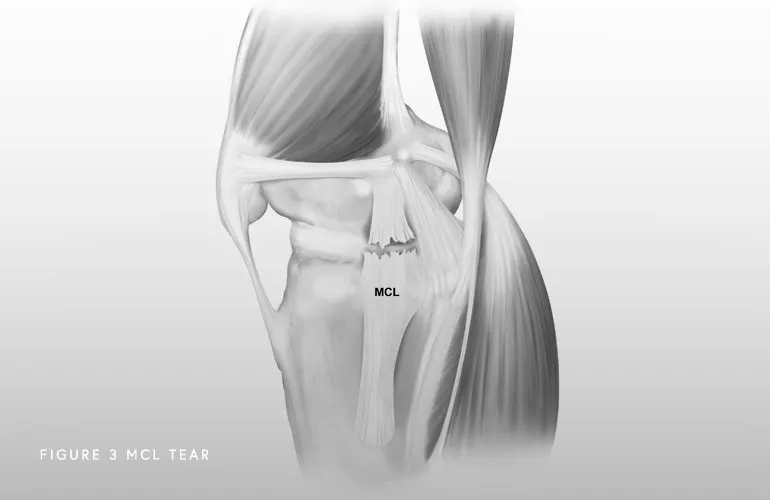
A combination of a comprehensive physical examination, special x-rays, and an MRI are usually very accurate. Dr. Bryan Penalosa and his team will perform a physical exam that will include testing your knee in an extended (straight) and flexed position to determine the location and severity of the injury. A special x-ray, called a valgus stress x-ray, will likely be obtained. This special x-ray allows Dr. Bryan Penalosa to objectively quantify and diagnose (based on validated systems) a posteromedial corner injury with millimeter accuracy. An MRI will allow Dr. Bryan Penalosa to further evaluate the extent of the MCL injury as well as to evaluate the knee for any concomitant ligament, meniscal, or cartilage injuries.
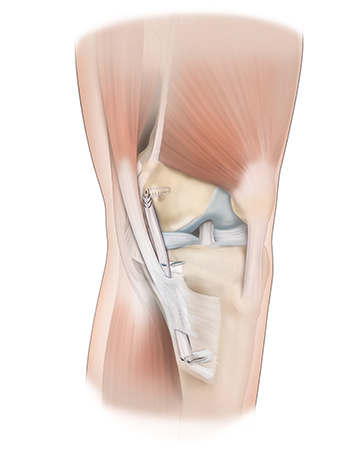
When there is a complete tear of the MCL (Grade 3) or when all the structures of the posteromedial corner of the knee are injured, surgery should be performed within two weeks after injury and once range of motion has been recovered. This is the best time to repair the structures because significant scarring and tissue weakening has not yet occurred. The position and alignment of the knee can also be anatomically restored during that time frame, rather than delaying and allowing the knee to heal in an abnormal position. Recent reconstruction techniques have allowed many patients to get back to high-level activities.
Restoring the native anatomy of the MCL and posteromedial corner can allow for early postoperative range of motion and produce better outcomes. There are multiple techniques described to do this, including augmentation procedures (meaning that a graft is utilized to supplement your own tissue) or full reconstruction. Full reconstruction includes use of a graft to reconstruct the MCL or all the components of the posteromedial corner (MCL and POL), depending on the degree of the injury.